Now We Have to Address Faulty Ideas about Immunity
______________
Where I am concerned, a new virus has become endemic when the severity is comparable to other viruses of its family. For coronaviridae, the best metric, in my judgment, to assess the status of a new virus is the CDC’s percentage of total deaths attributed to influenza and pneumonia (P&I). This is where deaths from coronaviruses would have been captured before the pandemic.
https://www.cdc.gov/flu/weekly/weeklyarchives2022-2023/data/NCHSData08.csv (retrieved 3-3-23)
Before the pandemic, this metric peaked between 7.6% and 10.9% during winters. The first two covid winters were far above this range (19.4% and 17.0%, respectively). This current winter, however, peaked at 9.2%, right in the middle of the pre-pandemic range. Despite covid, influenza, and other viruses co-circulating this winter, it has been an average winter in terms of respiratory mortality. This indicates that the severity of covid is now comparable to the endemic coronaviruses.
Why, then, has the U.S. recorded 300-600 covid deaths per day since December (or ~50,000 total since the start of cold and flu season in mid-October)? This is a higher number than what we would expect from endemic viruses. The answer, most likely, involves testing practices. It remains the standard practice to run a COVID-19 test on all patients admitted to the hospital. If a patient dies in the hospital with a positive covid test, COVID-19 will be listed as a cause of death (and thus added to the national figures), even if the patient was asymptomatic with respect to covid, or the patient had symptoms that would not have otherwise prompted doctors to test for viruses in the midst of other health issues.
Discussion of this subject is controversial given that, early in the pandemic, some people tried to use this reasoning to say that covid never posed a serious risk and that the covid death count was inflated by an order of magnitude. But there is a lack of evidence to substantiate that claim with respect to 2020-21, and as shown earlier, generic respiratory metrics showed an unusually severe situation. Now, however, the “with, not from” situation really is a big factor, and even some mainstream voices have started talking about it, such as Dr. Leana Wen: Dr. Leana Wen: Covid Numbers Have Been Overcounted; Deaths “With Covid” vs. “From Covid” | Video | RealClearPolitics.
Understanding how the current level of respiratory mortality is a sign of endemicity would help resolve the faulty ideas about immunity that have been propagated from many sides of the covid debate. On one side, we have people who believe that covid damages your immune system in a manner similar to HIV. Then in another camp, there are people who say that the covid vaccines damage your natural immune system (they have even coined the acronym VAIDS). The third problematic idea is the hypothesis of “immunity debt:” The idea that if people go for an unusually long time without exposure to viruses, they are merely deferring viral illnesses, which will eventually all occur in a short timespan when people are exposed to viruses again.
Let’s start with the theory that COVID-19 damages your immune system. On Twitter, I have already posted a link to an article by another blogger that does a good job of explaining the problems with the claims of immunosuppression. A key point made in the article was that “there is a very large and meaningful difference between *statistically significant* results with ultra-precise scientific instruments and *clinically significant* impacts at the population level.” So even if some experiments in laboratories showed T cell exhaustion/depletion after infection with SARS-CoV-2, that cannot tell us whether these findings affect clinical morbidity. Furthermore, we are lacking control studies to examine whether similar effects on cell mediated immunity occur temporarily after infections with endemic viruses.
The actual data from this winter has supported the aforementioned article’s suspicions about the immunosuppression claims. If covid is truly damaging the population’s immune systems, covid waves should become increasingly severe as reinfections occur. But there is no metric that shows a pattern of increasing severity. In addition to the pneumonia mortality statistics discussed earlier, consider the covid hospitalization trend:
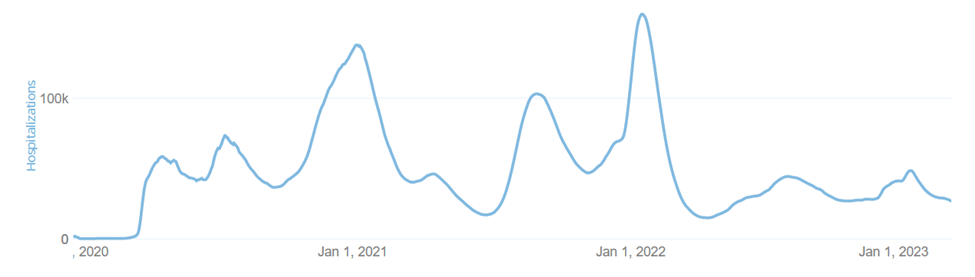
Source: United States – COVID-19 Overview – Johns Hopkins (jhu.edu) (retrieved 2-28-23)
Peak hospitalizations occurred in January 2022, when some regions of the U.S. still had a lot of immune naïve people (i.e. neither vaccine nor natural immunity), and the very contagious omicron variant was finding nearly all of them. Since then, reinfections have occurred as antibodies waned and omicron subvariants arose, but hospitalizations during the past 12 months have been nowhere near the Jan 2022 peak. This observation is particularly important because, if omicron subvariants evade antibodies, people will be relying on T and B cell immunity to avoid severe disease, and it is this very immunity that covid alarmists say is being damaged by covid!
Furthermore, these people claim that infection with covid confers no protection against reinfection (they are not confident in the vaccines to prevent infection either). If this were true, we would expect that as mutations occur to become theoretically more contagious, covid cases would hit new highs. But the actual caseload trend tells a different story:
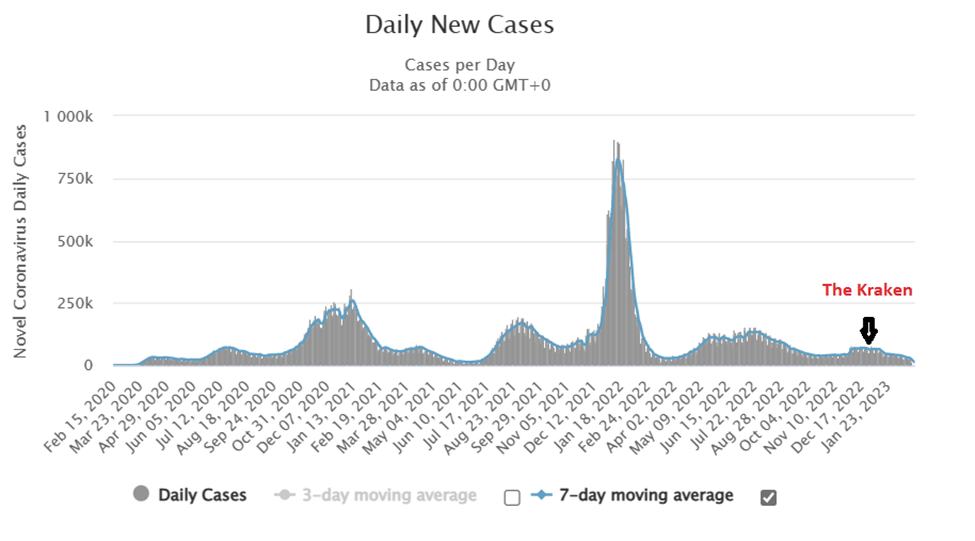
Source: United States COVID – Coronavirus Statistics – Worldometer (worldometers.info) (retrieved 2-28-23)
Cases peaked in January 2022, during the first omicron wave. Even though subsequent omicron subvariants have been theoretically more contagious, the waves have been much more subdued. In particular, the XBB subvariant hyped up as the “kraken” has been a dud. If these subvariants evade existing antibodies to the degree that the media reports, then the only way that cases can be subdued is for memory B cells to generate antibodies that are adapted to counter the new subvariant, and for memory T cells to recognize the subvariant as a familiar pathogen.
The bottom line is that the official statistics for cases, hospitalizations, and deaths, all indicate that cell mediated immunity in the American population is healthy and provides effective cross-immunity against omicron subvariants. This directly contradicts claims that covid infection confers no immunity, or that covid infection damages the immune system, or that the vaccines damage immunity.
There is, however, yet another faulty idea we have to contend with regarding immunity: The concept of “immunity debt.” This theory became prominent among critics of lockdowns, school closures, mask mandates, etc. The idea goes that, during the years when these public health mandates were in effect, people were not exposed to normal viruses, and that when these viruses eventually returned, people were unusually vulnerable to infection and illness because they had to catch up on their immunity to these pathogens.
The important thing to understand is that, when we are dealing with common types of pathogens such as coronaviruses, influenza, adenoviruses, etc., herd immunity from neutralizing antibodies only works in the context of a particular outbreak. When a new variant of these viruses emerges, it spreads rapidly through the population until the number of people who have acquired antibodies (combined with the people resistant to infection through other means) is large enough to protect those who have not been infected yet. When this happens, the rate of new infections declines and then stabilizes at a low level until the next mutation occurs, or antibodies wane.
The bottom line, however, is that this type of immunity is a short-term affair (a few months to a year). Beyond that, the reason the entire population does not get sick with new variants is that some people have cross-immunity from T and B cells (and perhaps robust generic functions) that prevents infection and/or illness. This immunity should not go away if you are shielded from viruses for a couple years.
Having said all of that, if people have not encountered a certain type of virus for a couple years, there is probably a modest increase in the chance of infection given the absence of antibodies. And that seems to be the case if we look at respiratory metrics for the recent winter:
First, here is the graph of influenza-like illness (ILI):
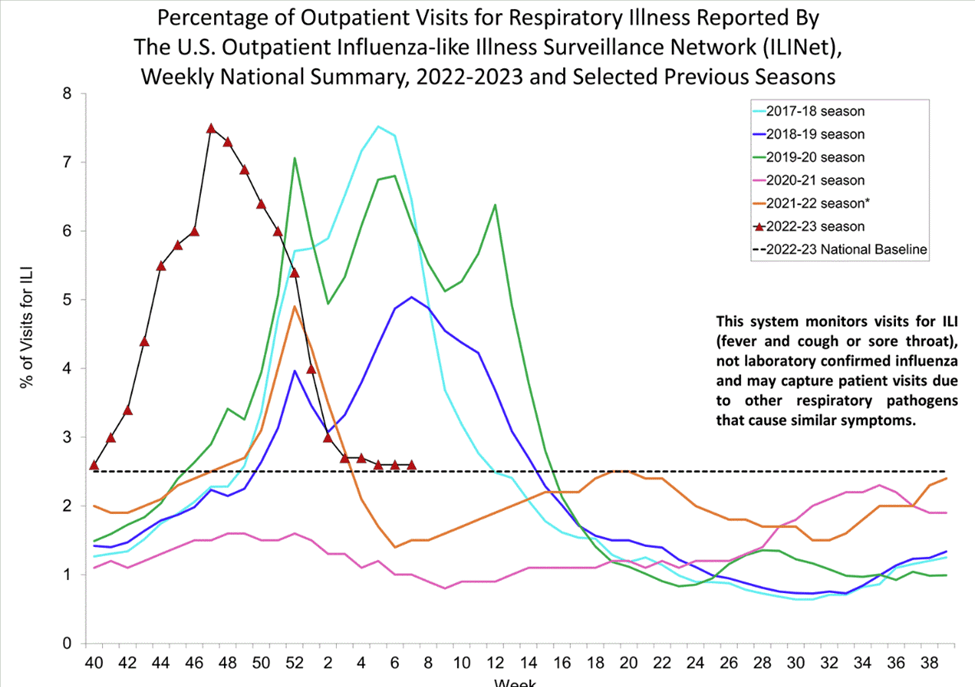
Source: cdc.gov/flu/weekly (retrieved 2-28-23)
As many anticipated, the lack of exposure to common cold and influenza pathogens for two years led to an above average season for 2022-23. But it was not an unprecedented surge. The peak level of flu-like illness was very close to 2017-18.
Here is the chart for influenza-confirmed hospitalizations:
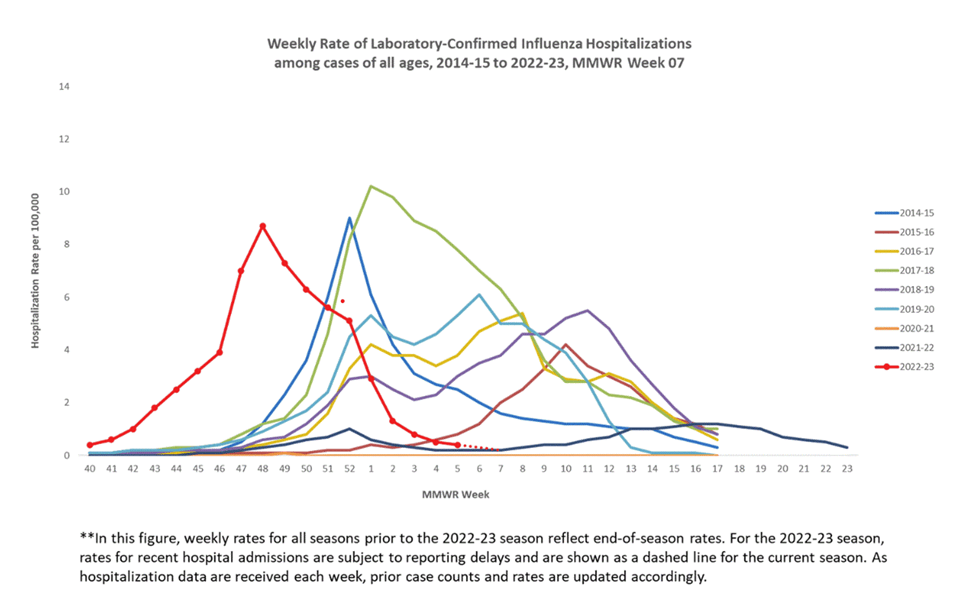
Source: cdc.gov/flu/weekly (retrieved 2-28-23)
Again, above average but not unprecedented. This season was most similar to 2014-15.
And as we saw earlier, mortality from influenza and pneumonia during this past winter was in the middle of the normal range.
Having considered fundamental immunology, and population-level respiratory illness metrics, I will now share personal experience that contradicts the “immunity debt” hypothesis. I have not had any viral illness since 2016. After a couple years without getting sick, I was not suddenly catching every virus out there. During the first year of covid, I was living a bubble lifestyle, and during the second year, I was mostly staying home because I didn’t know what I wanted to do. But ever since Spring 2022, I’ve been out and about, with plenty of opportunities to catch viruses if I were vulnerable to infection. In contrast to the “immunity debt” hypothesis, the day of reckoning has never come.
I am vaccinated against flu and covid (with all the boosters for my age), but I probably don’t have antibodies to many other viruses. But apparently, that doesn’t matter in my case. Cell mediated immunity is getting the job done. I am maintaining a healthy vitamin D level via supplementation, which likely helps in this regard. This past winter, I have also taken vitamin C and zinc at times, but given that I have never had a known deficiency in these, I cannot conclude that supplementation has reduced infection risk.
I am not saying that my six-year streak is possible for everybody, or that for me it will continue forever. But the idea that going for a couple years without viral illness makes you open to catching every bug on the planet is not something that my own experience testifies to, and it does not make sense from a standpoint of immunology either. I don’t think the people citing this hypothesis to support their anti-lockdown or anti-mask stance are helping their cause.
The good news at our present time is the strong evidence that covid has transitioned to endemicity. Now, the challenge for those of us interested in public health is to address faulty ideas about immunity. This serves two purposes. First, it will help calm down the virus anxiety that some people are still dealing with. Secondly, it will give way to knowledge about ways people can improve their immune functions, which will reduce the burden of endemic viral illness, and also make the population’s health more robust during future pandemics.
