Anyone who followed COVID-19-related news in 2020 was probably familiar with the controversies surrounding claims that certain existing drugs, most famously hydroxychloroquine and ivermectin, were effective at preventing severe disease from the SARS-CoV-2 coronavirus if administered early in the course of infection. Doctors who utilized such treatments faced censorship from social media platforms, unfavorable indexing of results on popular search engines, and sometimes even challenges to their medical licenses. The justification for such actions was the absence of randomized placebo-controlled trials demonstrating the efficacy of these drugs against COVID-19. But the censorship of these professionals obscured a fundamental flaw in the official narrative about COVID-19 and created a double-standard for the evidence required to promote interventions against the pandemic.
The official narrative about the new coronavirus SARS-CoV-2 was that this was a pathogen so foreign to the human immune system that if it ran through the population, massive numbers of hospitalizations and deaths would be unavoidable without a vaccine and antiviral treatments that target the virus. But from the early days of the pandemic, there were signs that this narrative was not exactly correct. For instance, it was widely acknowledged that 1/3 of all infections were asymptomatic. This should have been seen as evidence that the virus is not completely foreign to the human immune system, and should have prompted research into what enables the immune system to deal with this virus without wreaking havoc on mucous membranes. But instead, the asymptomatic infections and mild infections were used to amplify the fear of COVID-19; the virus was portrayed as some sort of especially devious, shape-shifting pathogen that can outsmart us.
But even among countries that had large COVID outbreaks in 2020, excess mortality rates varied widely. The website EuroMOMO has been tracking all-cause mortality rates in European countries for over a decade, and the mortality rates from country to country during 2020 paint vastly different images of the impact of COVID-19. For instance, consider the countries shown below:
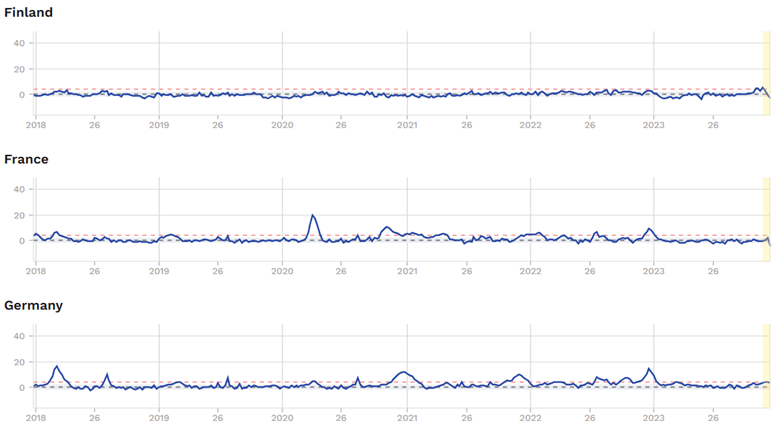
Source: https://www.euromomo.eu/graphs-and-maps/ (retrieved 12-26-2023)
Finland did not register any excess mortality at all during the entire pandemic period. France, on the other hand, had two waves of large excess mortality, one during Spring 2020 and another during Fall 2020. Germany had yet a different situation. They had an obvious wave of mortality during Fall 2020, but it was not as bad as their flu epidemic in 2018.
Here are four more countries:
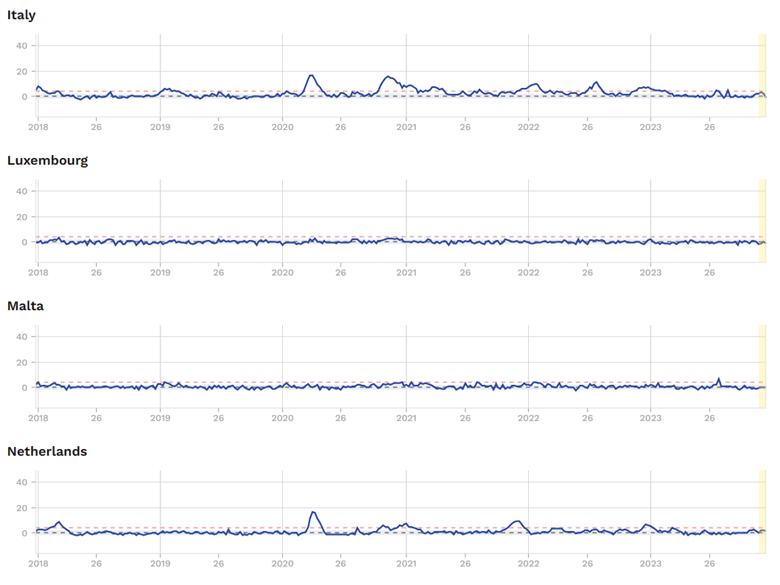
Source: https://www.euromomo.eu/graphs-and-maps/ (retrieved 12-26-23)
Italy had two severe waves of excess mortality, the first in Spring 2020 and the second in Fall 2020. In contrast, if you look at the graphs of Luxembourg and Malta, you would never know that a pandemic happened. The Netherlands has yet another type of situation. The first wave in Spring 2020 was severe. But the second wave in the fall-winter of 2020-21 was not any worse than the flu in 2018.
Now look at the four countries of the United Kingdom:
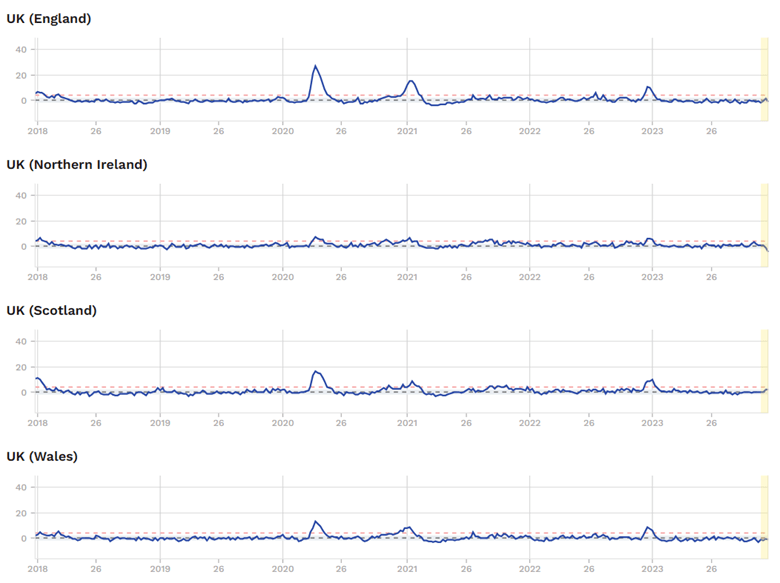
Source: https://www.euromomo.eu/graphs-and-maps/ (retrieved 12-26-23)
England had two severe waves of excess mortality, the first in Spring 2020 and the second in the winter of 2020-21.
Northern Ireland, on the other hand, exhibited minimal excess mortality throughout the entire pandemic period.
Scotland had one severe wave which occurred in Spring 2020. But the second wave in the winter of 2020-21 was milder than the flu in 2017-18.
Wales also had only one severe wave, occurring in Spring 2020. The second wave in the winter of 2020-21 only featured slight excess mortality.
Now, looking at the United States:
The USA was one of the countries with severe excess mortality during the COVID pandemic. Below is the graph from usmortality.com, covering the same period of time as the European graphs above:
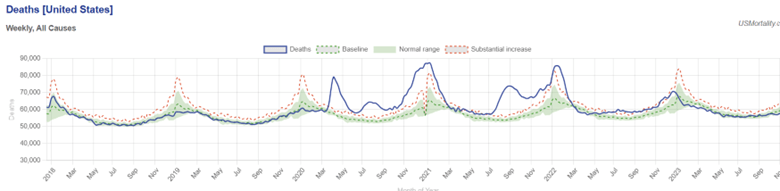
Source: https://www.usmortality.com/ (retrieved 12-26-23)
The USA had five waves of severe excess mortality. The first three were in Spring 2020, Summer 2020, and the fall-winter of 2020-21. Unlike the European countries we looked at, the USA had two additional waves of severe mortality: one in Summer 2021, then another in Winter 2021-22. The most likely explanation for this is the lower vaccination rates in the USA compared to Europe.
But even though the overall USA experienced severe excess mortality during the pandemic, there were doctors (considered highly reputable before the pandemic) who testified that they were not seeing fatal cases of COVID-19 in their practices (consisting of hundreds or thousands of patients) among patients who underwent their early treatment protocols. Among these doctors were Dr. Kelly Victory, a trauma physician, disaster preparedness specialist, and former Chief Medical Officer of Continental Airlines, Dr. Peter McCollough, a cardiologist and former vice chief of internal medicine at Baylor University Medical Center, and the doctors who operate the Front Line COVID-19 Critical Care Alliance (covid19criticalcare.com).
The criticism leveled at these physicians was that placebo-controlled studies on hydroxychloroquine and ivermectin did not demonstrate a reduction in severe cases of COVID-19. They then faced censorship and challenges to their medical licenses on the basis that they were promoting “medical misinformation.” But the censorship caused an important consideration to be overlooked: Even if the observational data from these physicians do not prove a particular drug to be beneficial, the fact that these physicians were not seeing the hospitalization and fatality rates among their patients which were observed in the general population, is yet another type of evidence demonstrating that the SARS-CoV-2 coronavirus does not have to cause mass hospitalization and death in the absence of vaccines and antiviral drugs.
Many of these doctors promoting “early treatment” were also using supplements such as vitamin D, vitamin C, zinc, and quercetin. These supplements have immunomodulatory effects that help the immune system fight viruses in a way that minimizes tissue damage. It is possible that it is these supplements, rather than the prescription medications, that prevented severe disease in these patients. It is also possible that the use of these supplements enabled hydroxychloroquine or ivermectin to have beneficial effects that would not have occurred otherwise.
It is also possible that patients treated by these physicians had good outcomes because they were not given certain harmful treatments. The only type of treatment that mainstream doctors believed was beneficial against COVID-19 was steroid therapy, in particular dexamethasone. The reason was that these drugs reduce inflammation in the lungs. However, they do so by suppressing immune functions which can give way to bacterial superinfections and also enable the virus itself to cause more damage to organs.
For this reason, steroids are not normally used in patients hospitalized with viral illnesses. But in the case of COVID-19, these drugs were administered whenever covid-positive patients had difficulty breathing. The German physician Dr. Claus Köhnlein has been a vocal critic of the use of steroids to treat COVID-19. Here are two videos in which he was interviewed about the pandemic, as well as his response to other viral diseases:
https://odysee.com/@drsambailey:c/pcr-pandemic-interview-with-virus-mania:9
https://odysee.com/@PlanetLockdown:6/Claus-Ko%CC%88hnlein-office:a
Some “early treatment” proponents in the United States did use steroids in their protocols. But the negative effects of steroids on the immune system may have been offset by positive effects from vitamin supplements, hydroxychloroquine, or ivermectin. Furthermore, many of these “early treatment” protocols included antibiotics, which may have prevented bacterial superinfections while on steroid therapy.
In the case of Dr. Köhnlein, he has been taking a critical look at the causes of viral epidemics for over 30 years, beginning with HIV/AIDS. While the official narrative was that HIV would always cause AIDS (and consequently death) in the absence of antiviral therapy, Dr. Köhnlein concluded that this was not the case after studying the early writings on HIV and the circumstances of AIDS patients. He found that the major contributors to AIDS mortality were recreational drugs with immunosuppressive effects used by homosexual men and heterosexual drug addicts, and excessive, immunocompromising doses of the chemotherapy-like drug AZT that were used to treat HIV-positive people in the late-1980s and early-1990s.
Since 1993, he has operated a private practice on Kiehl, Germany, in which he helps HIV-positive and hepatitis-positive patients live normally with only temporary use, or no use, of antiviral drugs, by advising them on diet and lifestyle to promote their immune health. It may not come as a surprise, then, that he has not seen severe cases of COVID-19 among his patients, given their immune health. While he has not denounced the use of hydroxychloroquine or ivermectin, he does not use them in his practice as he does not deem them necessary. This is further evidence that the human immune system has the capability to deal with SARS-CoV-2 (and other types of “new viruses”) and could support the idea that it was immune support, not prescription drugs, that enabled the American physicians promoting “early treatment” to see better outcomes among their patients than the population at large.
But returning to the subject of censorship, the problem is that censorship made it impossible to answer these questions definitively. Throughout history, science has advanced despite some theories and models not being exactly correct. If every scientific and medical claim that was problematic in some way had been censored, we would still be in the dark ages. Critical thinking and analysis, rather than absolute correctness every step of the way, is what drives science forward. A claim can be flawed, yet still be an intermediate step that leads to important discoveries.
Another problem caused by censorship during COVID-19 was that it created a double-standard for the proof of efficacy required to promote pandemic interventions. Mitigations such as community mask-wearing and social distancing were presented as unquestionable ordinances, even though studies with control groups at the population level were rarely conducted, and when they were, the results often did not show a significant reduction in infection rates among the intervention group. For instance, here is a discussion by Dr. John Campbell on a large study on community masking:
This is not to say that nobody ever avoided infection by wearing a mask or keeping physical distance. Rather, it simply indicates that there was not a basis to claim that these interventions were the keys to “flattening the curve” of COVID-19. A double standard arose because the type of proof demanded by the establishments for hydroxychloroquine, ivermectin, and vitamin supplements was never demanded for masking and social distancing.
And there’s a similar double standard involving Paxlovid. While there was a placebo-controlled trial which showed a significant reduction in hospitalization among patients who took the drug, the trial was conducted on unvaccinated adults during the period of the Delta variant. Subsequent trials conducted on vaccinated populations during the Omicron period have not shown better outcomes in the Paxlovid group. Nevertheless, health agencies in the U.S. and Europe are still recommending Paxlovid to any “high risk” people who test positive for COVID-19. Here is a link to a discussion by Dr. Vinay Prasad on Paxlovid studies:
https://youtu.be/4wDRva5O0v0?si=HdzBA2DRuSL8xxtj (Paxlovid discussion starts at 10:25).
Now, it is quite plausible that, for some vaccinated individuals infected with Omicron, Paxlovid has been beneficial. Observational studies have had positive results, but such studies had positive results for hydroxychloroquine and ivermectin as well.
What has become apparent over the last four years is that censorship has not been carried out in an even-handed manner. It cannot be said that censorship has served the purpose of holding science and medicine to the highest standards. Contrary to the mainstream media’s concern, the biggest problem of our time is not wrong information per se. Rather, it is the manipulation of public discourse which further polarizes society by making it easy to blame all of society’s problems on those who dissent from accepted narratives. Furthermore, even certain information that may indeed be flawed, could nevertheless reveal problems with prevailing narratives and be a launching point for investigation into what is really going on.
I think that what all of us can agree upon is that the COVID-19 pandemic impacted the average, random person on this planet, as well as the medical community, to a degree that surpasses any other circumstance in our lifetimes. As such, COVID-19 has enabled us to see the impact of government and Big Tech involvement in public and scientific discourse to an extent that was not possible before 2020. As such, it is not a stretch to suspect that the problems affecting such discourse on COVID-19, are also affecting discourse on other controversial issues. It is due time for people to consider the “other side” of the debate on many issues, not to determine if it is absolutely true and worthy of loyalty, but rather, to see if it reveals any issues with one’s existing way of looking at the matter.

One response to “The Early Treatment Quandary and the Harm Caused by Censorship”
[…] later), the populations as a whole appear to have benefitted from covid vaccination. In my article here, I show graphs of excess mortality trends from the website EuroMOMO. In Western European countries […]
LikeLike